PREACH Implementation Project – A Socio-Ecological framework for Hypertension in Pakistan
Background
The latest estimate suggest that 1.4 billion people are living with hypertension globally1 and World Health Organization (WHO) predicts hypertension shall affect 1.6 billion people across the world by 2025, approx. 29% of world’s population.2 Moreover, worldwide, hypertension is estimated to cause 7.5 million deaths, about 12.8% of the total of all deaths. This accounts for 57 million disability adjusted life years (DALYS) or 3.7% of total DALYS.3
It is alarming that, fifty-four percent of strokes and forty-seven percent of cardiovascular deaths are caused by suboptimal control of blood pressure.4 By the time hypertension patient is diagnosed at tertiary care hospital, there is already one organ damage involved. According to national health survey (2010), 33% of adults aged 45 years and 18% of all adults in Pakistan were hypertensive, and every third hypertensive aged 40 years and above was susceptible to an extensive range of diseases. This survey also revealed that only half of the diagnosed hypertensive subjects were treated at any time, making the prevalence of controlled hypertension only 12.5%.5 Hypertension knowledge in hypertensive patients is not adequate and is alarmingly poor in patients with uncontrolled hypertension.6
One of the reasons of unsatisfactory clinical management of disease is a lack of standardized approach across Pakistan. A National Standardized Guideline is needed for Public Sector (30% of Patients)7 to address the issue of varying clinical practices. Developing country does not have resources to manage complications of hypertension leading to stroke, MI, HF, etc. Therefore, early surveillance and community screening is the ONLY means to detect early onset of hypertension. (Possibly 10 – 15 years can be added before organ damage shows up). A more cost-effective strategy probably for the country is to reduce the burden on tertiary care hospitals and to make GPs as first line respondents. BP control can only be achieved if those with hypertension are identified, diagnosed, and treated timely at community level.
The alarming situation of deteriorating state of Pakistan’s economic and health infrastructure demands concrete measures to be taken. Therefore, Getz Pharma takes pride in launching a project called PREACH ‘Prevention, Management and Control of Hypertension’ aiming to ignite a paradigm shift from tertiary hospitals to primary care facilities and from treatment alone to preventive care. Additionally raising awareness in the general masses and developing a trained force to battle against this silent killer – hypertension.
Goal
Reducing the burden of hypertension from tertiary care to primary care and from specialist to general practice.
Objective
The primary objectives of PREACH are the following:
- Train the registered healthcare practitioners on standard national guidelines through the train the trainer model
- Educate & Aware the individual and community at large for home blood pressure monitoring
- Mapping and advising for self-referral pathway
- Forming a National Hypertension Registry
- Establishing an enabling environment for inclusion of hypertension in essential primary package
PREACH Implementation Plan – Multi-sectorial Strategy (Figure 1)
Supply
- A standardized curriculum and assessment forms will be prepared derived from the updated national hypertension guidelines.
- A capacity building training of registered doctors (senior & young consultants, family physicians, and general practitioners) across Pakistan on standard curriculum.
- Simultaneously impact assessment studies will be carried out to evaluate the effectiveness of PREACH project.
Demand creation & Community Awareness
- A scientific study will be conducted with academic partner to identify and create easiest methods for diagnosis of hypertension through home blood pressure monitoring.
- A standard mass grassroots level awareness drive will be developed to aware individuals and community on hypertension screening and home blood pressure monitoring.
- Self-screening and self-referral pathway & mapping of GP’s for timely diagnosis and management of hypertension.
Enabling environment
- Discuss with Government officials to include project PREACH in annual development programs and for budget mobilization.
- Doing advocacy for policy inclusion of hypertension in primary care package.
- Generating funds from local and international bilateral/multilateral donors.
National Hypertension Registry
- Development of a national hypertension registry for robust data collection, analytics, and evidence based publications for informed clinical decisions.
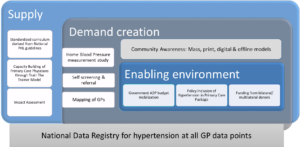
Figure 1: Implementation Model of Project PREACH
The Socio-Ecological model of project PREACH – A framework for the prevention of Hypertension in Pakistan (Figure 2)
The PREACH project is designed with an approach to bring a change on population level with integration of all societal level determinants that influence the hypertension for e.g.: physician-patient gap in healthcare service delivery, lack of early screening and diagnosis of hypertension on primary level.
Therefore, the first pivot is bringing change on individual level by encouraging people to self-screen themselves at home and self-refer themselves to trained practitioner. Simultaneously, the general practitioner workforce will be trained to standardize the health services (hypertension treatment) in the community. The idea is to create demand from the community through self-referral to GP and from there to tertiary care level and supply it by building the capacity of health practitioners via train the trainer model which includes cascade down training session resulting in a workforce ready to defeat hypertension.
After achieving this milestone, the project’s objective is to build a 1st national data registry on hypertension resulting in building a database of patient which will enable the policy maker to devise particular action plans and targets for the prevention of hypertension disease in Pakistan. Furthermore, building strong liaison with policy advisors to advocate on bringing hypertension to essential healthcare package of Government of Pakistan for NCD’s.
With this framework, the aim is to synergize multiple sectors to come forward and work towards one approach i.e. to reduce the hypertension burden in Pakistan.
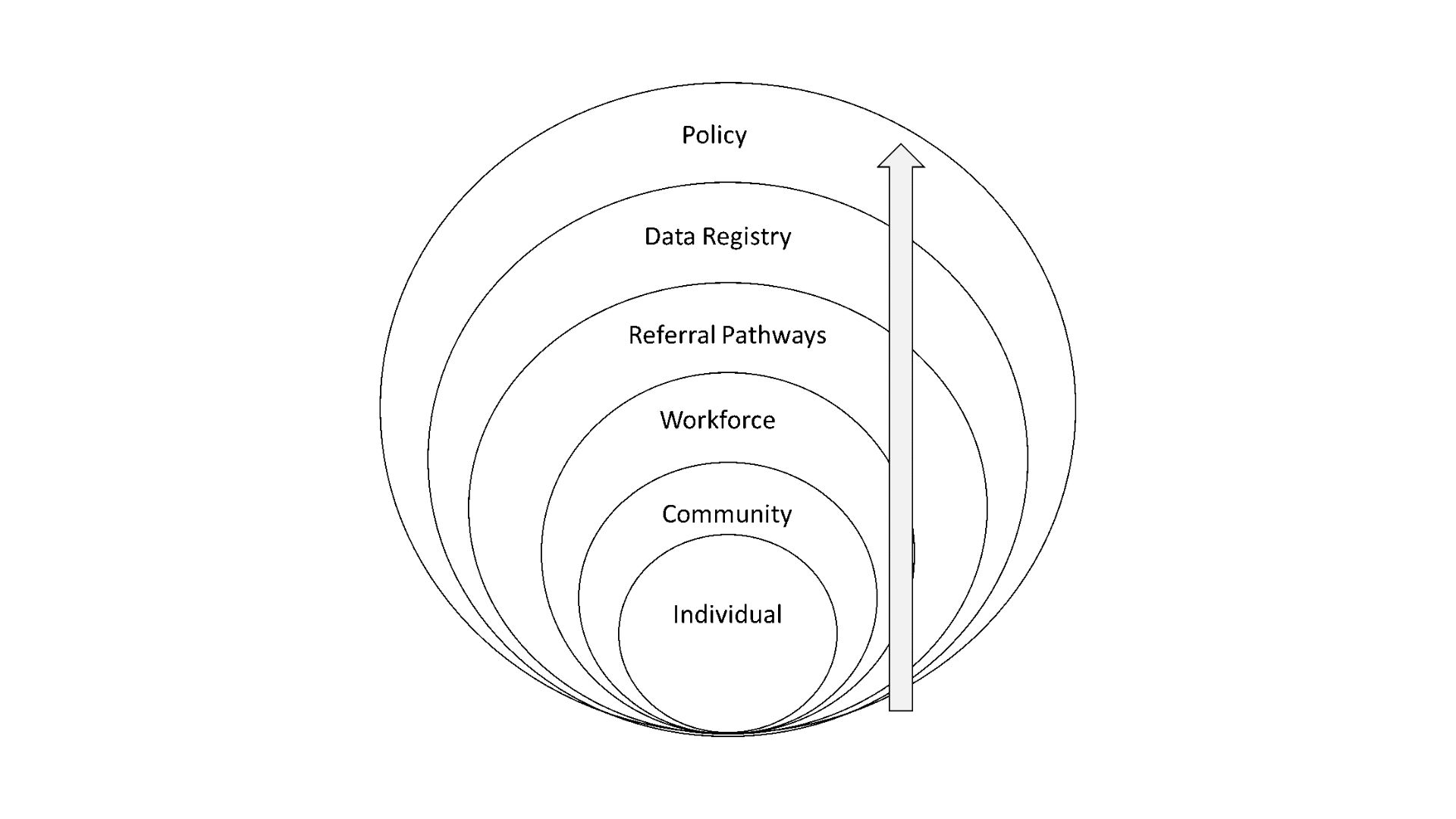
Figure 2: 6 step Socio-Ecological model adapted for project PREACH
Note: The socio-ecological model is excerpted from cdc.gov and modified for the PREACH project.
Read the article here: https://ojs.jpma.org.pk/index.php/public_html/issue/view/57
References:
1. High blood pressure – measure accurately, control it and live longer (who.int)
2. Riaz M, Shah G, Asif M, Shah A, Adhikari K, Abu-Shaheen A. Factors associated with hypertension in Pakistan: A systematic review and meta-analysis. PloS one. 2021 Jan 29;16(1):e0246085.
3. https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3155
4. Nadeem MK, Mari A, Iftikhar S, Khatri A, Sarwar T, Patel MJ. Hypertension-related Knowledge and Its Relationship with Blood Pressure Control in Hypertensive Patients Visiting a Semi-private Tertiary-care Charity Hospital in Karachi, Pakistan. Cureus. 2019 Oct;11(10).
5. Saleem F, Hassali AA, Shafie AA. Hypertension in Pakistan: time to take some serious action [published correction appears in Br J Gen Pract. 2010 Jul;60(576):536. Dua, Jalan Sungai [removed]]. Br J Gen Pract. 2010; 60(575):449–450.
6. Almas A, Godil SS, Lalani S, Samani ZA, Khan AH. Good knowledge about hypertension is linked to better control of hypertension; a multicentre cross sectional study in Karachi, Pakistan. BMC research notes. 2012 Dec;5(1):1-8
7. Naz L, Ghimire U, Zainab A. Behavioral factors associated with utilization of healthcare services among elderly in Pakistan: evidence from a nationally representative survey. BMC Geriatr. 2021 Jan 12;21(1):42. doi: 10.1186/s12877-021-02005-3. PMID: 33435874; PMCID: PMC7802143.
Authors:
Dr. Wajiha Javed
Jaffer Bin Baqar
Samra Maqbool
Public Health & Research Department, Getz Pharma
Corresponding author:
Dr. Wajiha Javed, email: [email protected]
Mailing Address: 29-30/27, Korangi Industrial Area, Karachi 74900, Pakistan